


DIABETIC RETINOPATHY
DIABETIC RETINOPATHY
It is the “disease of the retina” caused by microangiopathy due to long term effect of diabetes leading to progressive damage of the retina & blindness.
Most common cause of severe bilateral visual loss in working age group.
Risk Factors
- Age at diagnosis of diabetes
- Duration of diabetes
- Poor metabolic control
- Pregnancy
- Hypertension
- Nephropathy
- Others – smoking, obesity, hyperlipidemia, anemia
Pathophysiology
- Diabetic Retinopathy is a microangiopathy primarily affecting the precapillary arterioles, capillaries,
venules and post capillary venules. - The basic component of damaging process are microvascular occlusion & microvascular
leakage.

Capillary Changes
- Degeneration & loss of pericytes
- Thickening of Basement membrane
- Damage & proliferation of endothelial cells
Hematological Changes:
- Deformation of RBC & rouleaux formation
- Increased plasma viscosity
- Increased platelet stickiness & aggregation






Microaneurysm
- Earliest sign of Diabetic Retinopathy.
- Appear as tiny red dots.
- It is focal saccular dilatation of capillary walls where pericytes are absent.
- Located in the outer plexiform layer & inner nuclear layer.
- Usually at posterior pole, especially temporal to the fovea.
- In FFA — present at the edge of area of capillary non- perfusion (hyper fluorescence dots)
Dot & Blot Haemorrhage:
- Due to rupture of wall of capillary or microaneurysm, giving rise to intra retinal haemorrhage.
- If the haemorrhageis deep (i.e. in the inner layer of Outer Plexiform Layer) it is usually is round or oval (dot/ blot haemorrhage)


Flame Shaped Haemorrhage
- Arise from superficial precapillary arterioles.
- The haemorrhage is more superficial & in the nerve fiber layer, it takes a flame/ splinter shape as it follows the architecture of the nerve fiber layer.
Exudates
Hard Exudates:
- These are yellow deposits of lipid, lipoprotein & lipid filled macrophages within the outer plexiform & inner nuclear layer.
They are arranged in clumps or form circinate pattern around the macula frequently at posterior pole. - These are signs of current/previous Macular edema.
Cotton wool Spot (soft exudates):
- They are white fluffy lesions in the
nerve fiber layer. - Caused by capillary occlusion at
nerve fiber layer due to infarction.

Intraretinal microvascular abnormality (IRMA):
- Abnormal dilated, tortuous retinal capillaries that act as a shunt between arterioles & venules.
- It’s located within the internal limiting membrane.
Venous changes:
- In the form of “beading”, “looping” & “severe segmentation” due to venous stagnation.

CLASSIFICATION
ETDRS CLASSIFICATION:- NON PROLIFERATIVE DIABETIC RETINOPATHY
ETDRS CLASSIFICATION:- NON PROLIFERATIVE DIABETIC RETINOPATHY
| MILD NPDR | micro aneurysms, retinal hemorrhage, hard exudates |
| MODERATE NPDR | Mild NPDR plus cotton wool spots, venous changes & IRMA |
| SEVERE NPDR 4:2:1 rule | Moderate NPDR plus one of — micro aneurysms, retinal haemorrhage in all four quadrants Venous changes in 2 or more quadrants IRMA atleast in 1 quadrant |
| VERY SEVERE NPDR | Two or more of the above features on severe NPDR |
Proliferative Diabetic Retinopathy:
early/ mild/ non — high risk PDR
High Risk:
◉ New vessel on Disc:
- More than 1/3rd of Optic disc diameter with/ without haemorrhage
- Less than 1/3rd of optic disc diameter with haemorrhage (preretinal & vitreous haemorrhage)
◉ New vessel Elsewhere in Fundus:
- More than 1/2 or equal to 1/2 of Optic disc diameter with/ without haemorrhage
- Less than 1/2 of Optic disc diameter with haemorrhage. (preretinal & vitreous haemorrhage)

Clinically Significant Macular Edema
Modified Airlie- House criteria:
- Retinal edema within 500 micron of central fovea
- Hard Exudates within 500 micron of fovea centralis associated with adjacent retinal thickening
- Retinal edema that is 1 disc diameter or larger, any part of which is with in 1 disc diameter of the fovea centralis.
Why us at IClinix Diabetic Eye Care?
- Advance eye scan for people for all
- Captures digital photograph of layers of the retina
- Easy and Painless
- Can monitor the progression of any changes in your retina


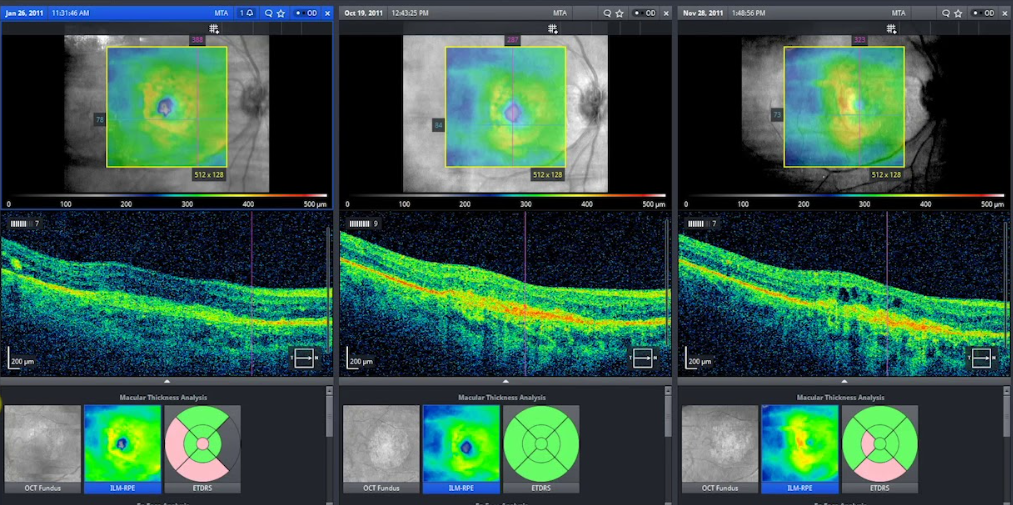
ZEISS RETINA WORKPLACE:
see your retina profile evolve over years under ICLINIX and compare yourself how the disease is controlled. We bring the FORUM for your individualised follow ups
- Visualize integrated imaging data in seconds
- Rapid and comprehensive: Fully assess retinal structure in seconds
- Enhanced diagnosis and prognostication
MINIMALLY INVASIVE VITREORETINAL SURGERY (MIVS)
- Advanced Sutureless Vitrectomy/ Minimal Gauge Vitrectomy
- Faster Recovery
- Zero Astigmatism



